
Home / What is Myopia?What is Myopia — And Why Does It Matter?
Myopia is more than just needing glasses. Understanding what's happening inside your child's eyes is the first step to protecting their long-term vision.
Myopia in Simple Terms
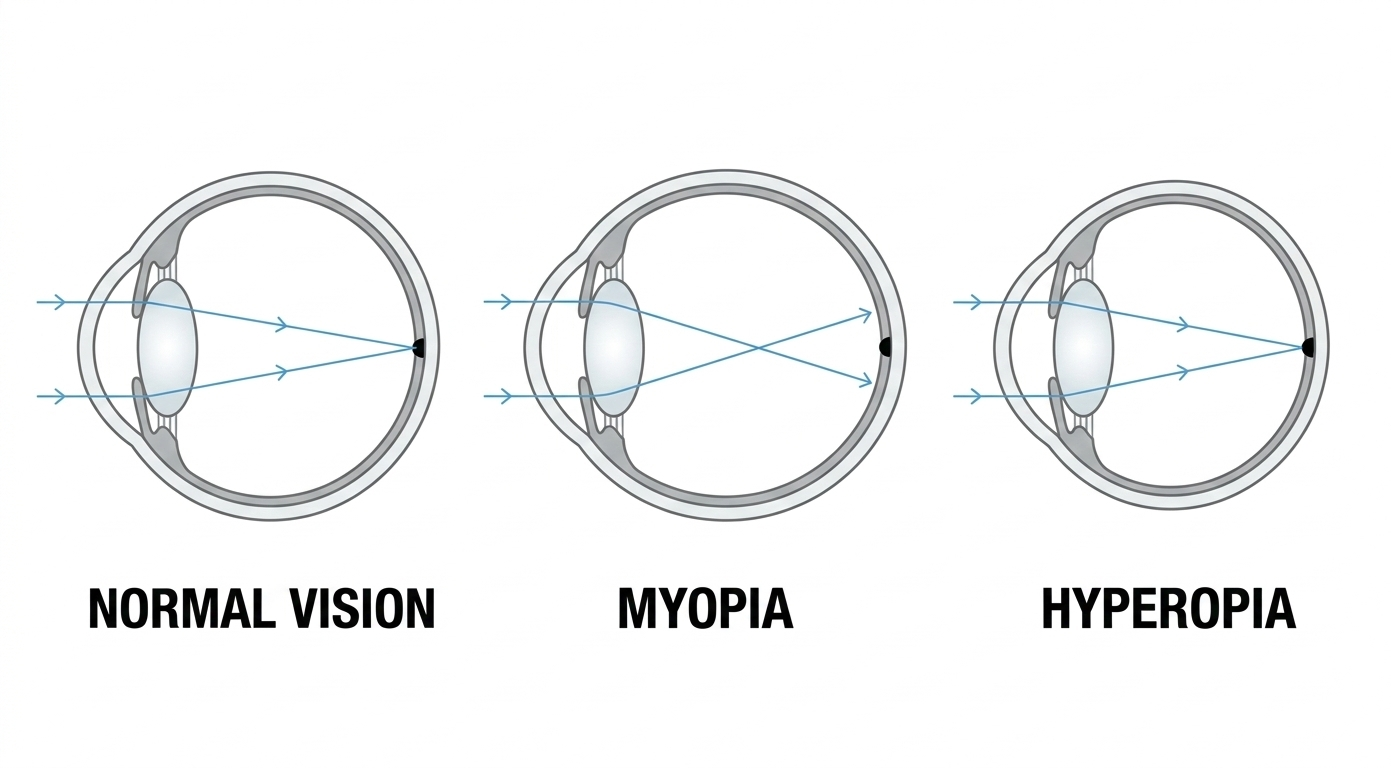
Myopia — commonly called short-sightedness or nearsightedness — is a vision condition where distant objects appear blurry while close objects remain clear.
It happens when the eyeball grows too long from front to back. Light entering the eye focuses in front of the retina instead of directly on it, causing distance blur.
Glasses and contact lenses correct the blur by refocusing light onto the retina. But they don't address the underlying problem: the eye is still too long, and in most children, it keeps growing.
Why Myopia Progresses
In most children, myopia isn't a one-time diagnosis — it's a progressive condition. The eyeball continues to elongate throughout childhood, and with each millimetre of growth, the prescription gets stronger.
The pattern is predictable:
Most myopia develops between ages 6–16
Younger onset typically means faster progression
Without intervention, prescriptions increase by an average of -0.50D per year
Progression usually slows in the late teens as eye growth stabilises
What drives progression?
The exact mechanisms are still being researched, but we know several factors contribute:
Genetics
Children with myopic parents are significantly more likely to develop myopia. Two myopic parents increases the risk substantially compared to one or none.
Near Work
Extended time spent on close-focus tasks — reading, screens, homework — is associated with myopia development and progression.
Limited Outdoor Time
Research consistently shows that children who spend more time outdoors have lower rates of myopia. The protective effect appears related to light exposure, not physical activity.
Visual Environment
Modern lifestyles involve more indoor time, more screens, and more near work than previous generations. This environmental shift correlates with rising myopia rates worldwide.
Risk Factors for Developing Myopia
For children who don't yet have myopia, several factors predict whether they will develop it. These can be grouped into non-modifiable factors (which help us identify at-risk children) and modifiable factors (which you can act on).
Non-Modifiable Risk Factors
These factors can't be changed — but knowing them helps us monitor closely and act early.
Certain Binocular Vision Issues
Children with esophoria (eyes tending slightly inward) and high AC/A ratios have a dramatically increased risk of developing myopia within one year.1-3 These issues can only be detected through a comprehensive eye examination.
Two Myopic Parents
If both parents are myopic, the child's risk increases six-fold.4 Combined with low hyperopic reserve, only 23% of these children avoid myopia by their teenage years.5
One Myopic Parent
Having one myopic parent triples the risk of a child developing myopia compared to children with no myopic parents.4
Low Hyperopic Reserve
The single most significant independent predictor. Children with less than +0.75D of hyperopia at age 6–7 are highly likely to become myopic by their teens — regardless of family history or lifestyle.5
Intermittent Exotropia
This binocular vision condition (where one eye occasionally turns outward) is strongly associated with myopia. Research shows 50% of children with IXT are myopic by age 10, and 90% by age 20.6
Modifiable Risk Factors
These are the factors you can influence. They're your action points.
Limited Outdoor Time
Children who spend less than 90 minutes per day outdoors are at increased risk.7,8 This is the single most evidence-based lifestyle intervention. Aim for at least 2 hours daily — the protective effect comes from light exposure, not exercise.9
Excessive Near Work
More than 3 hours of close-focus activities outside school time increases risk, especially combined with limited outdoor time.10 Reading, screens, and homework all count. Risk increases by approximately 2% for every additional diopter-hour per week.
Risk Factors for Faster Progression
Once a child is myopic, different factors determine how quickly their prescription increases. Understanding these helps us tailor treatment intensity.
Non-Modifiable Progression Factors
Younger Age of Onset
Children who become myopic at age 7 typically progress by at least -1.00D per year. This rate approximately halves by age 11–12 as eye growth naturally slows.11 This is why early intervention matters most.
Family History
Children with two myopic parents are the fastest progressors.12 Children with highly myopic parents (over -6.00D) are more likely to progress to high myopia themselves.13
Higher Baseline Myopia
Children who are already more myopic at diagnosis tend to progress faster.14 This is why early detection matters — catching myopia early means starting from a lower prescription.
East Asian Ethnicity
Research shows East and Southeast Asian children tend to progress faster than children of European descent.15,16 However, myopia control treatments are equally effective regardless of ethnicity.17
Modifiable Progression Factors
Close Working Distance
Reading or using devices at less than 20cm has been linked to faster progression.18 Encourage your child to hold books and screens at arm's length — the "Harmon distance" (elbow to knuckle) is a good guide.
Prolonged Continuous Near Work
Sessions longer than 30–45 minutes without a break are associated with faster progression.18 The 20-20-20 rule helps: every 20 minutes, look at something 20 feet (6m) away for 20 seconds.
Outdoor Time
While the evidence is stronger for preventing onset than slowing progression, outdoor time remains best practice.9 Continue aiming for at least 2 hours daily.
No Myopia Control Treatment
Standard single-vision glasses correct blur but don't slow progression. Evidence-based myopia control treatments reduce progression by 50–60% on average.19 Starting treatment is the most impactful modifiable factor.
What This Means For Your Child
Some Risks Require Professional Detection
The highest-impact risk factors — binocular vision issues and low hyperopic reserve — can only be identified through a comprehensive eye examination. This is why regular childhood eye tests matter, especially with family history.
You Can't Change Genetics — But You Can Act Early
Family history, age, and ethnicity aren't changeable. But knowing your child has these risk factors means you can monitor more closely and start treatment earlier if myopia develops.
Outdoor Time is Your Best Prevention Tool
Increasing outdoor time to at least 2 hours daily is the most evidence-based lifestyle intervention for reducing myopia risk.7-9 It's simple, free, and has benefits beyond vision.
Earlier Onset = More Urgent Action
If your child develops myopia young, they will progress faster.11 This is precisely why starting myopia control treatment early makes such a difference to the final outcome.
The Real Risk: High Myopia
Many parents assume myopia just means thicker glasses. The reality is more serious.
High myopia — typically defined as -5.00D or greater — significantly increases the lifetime risk of sight-threatening eye conditions:
Retinal Detachment
The retina pulls away from the back of the eye — a medical emergency requiring immediate surgery. High myopes are 5–6× more likely to experience this.
Myopic Macular Degeneration
Damage to the central vision area from stretching of the eye. A leading cause of blindness in highly myopic adults. No cure exists.
Glaucoma
Increased eye pressure damages the optic nerve, causing progressive vision loss. Risk is 2–3× higher in high myopes.
Early Cataracts
Clouding of the eye's lens typically occurs earlier in myopic eyes, often requiring surgery in middle age rather than later life.
These risks increase with every dioptre of myopia. A child who reaches -6.00D faces significantly higher lifetime risk than one who stabilises at -3.00D. Every dioptre we prevent matters.
When Should Myopia Control Start?
The short answer: as early as possible.
Myopia control is most effective when started early — ideally at first diagnosis or when risk factors are identified. The goal is to slow progression during the critical years (ages 6–16) when the eye is still growing.
Pre-Myopia Screening
Children with risk factors (family history, low outdoor time) should be monitored even before myopia develops. Early detection allows earlier intervention.
Ideal Intervention Window
If myopia is diagnosed, this is the optimal time to begin myopia control. Starting early means more years of slowed progression and a lower final prescription.
Still Highly Effective
Myopia control remains very effective through the pre-teen years. Most children in this range are good candidates for Ortho-K, MiyoSmart, or MiSight.
Worth Starting
Progression often continues through the mid-teens. Even a few years of myopia control can make a meaningful difference to the final prescription.
Monitoring Phase
Myopia typically stabilises in the late teens. We continue monitoring and can adjust or taper treatment as progression slows.
How We Slow Myopia
Several evidence-based treatments can slow myopia progression by 50–60%. The best choice depends on your child's age, prescription, and lifestyle.
Ortho-K
Custom night lenses reshape the cornea while sleeping. Wake up with clear vision — no glasses or contacts during the day.
Up to 60% slower progression Learn more →MiyoSmart Glasses
Specially designed lenses that look like normal glasses but actively slow eye growth. The simplest option for younger children.
Up to 60% slower progression Learn more →MiSight Contacts
FDA-approved daily disposable lenses worn during the day. Great for active kids who want freedom from glasses.
Up to 59% slower progression Learn more →Atropine Drops
One drop at bedtime slows progression. Often combined with other treatments for enhanced control.
Up to 50% slower progression Learn more →Not sure which is right for your child? That's what the assessment is for. We'll evaluate your child's eyes, discuss their lifestyle, and recommend the best approach.
Common Questions
Is myopia the same as short-sightedness?
Yes — myopia, short-sightedness, and nearsightedness all describe the same condition. Distance vision is blurry, near vision is clear.
Will my child grow out of it?
No. Myopia doesn't reverse on its own. Without intervention, it typically continues to progress until the late teens when eye growth stabilises.
Can screen time cause myopia?
Excessive near work (including screens) is associated with myopia progression, but the relationship is complex. Outdoor time appears more protective than limiting screens alone.
How much outdoor time is recommended?
Research suggests at least 90–120 minutes of outdoor time daily helps protect against myopia development. The protective effect comes from light exposure.
Do regular glasses make myopia worse?
No — and not wearing glasses doesn't slow progression either. Standard single-vision glasses simply don't affect progression one way or the other. Myopia control treatments are specifically designed to slow it.
Is myopia control guaranteed to work?
No treatment guarantees zero progression, but clinical evidence shows 50–60% slower progression on average. Some children respond better than others.
Book a myopia assessment with Dr Mark Joung. We'll measure your child's current prescription, assess their risk factors, and create a plan to protect their vision.
Find Out Where Your Child Stands
References
- Goss DA, Jackson TW. Clinical findings before the onset of myopia in youth: 3. Heterophoria. Optom Vis Sci. 1996;73(4):269-278.
- Mutti DO, Mitchell GL, Jones-Jordan LA, et al.; CLEERE Study Group. The Response AC/A Ratio Before and After the Onset of Myopia. Invest Ophthalmol Vis Sci. 2017;58(3):1594-1602.
- Gwiazda J, Thorn F, Held R. Accommodation, accommodative convergence, and response AC/A ratios before and at the onset of myopia in children. Optom Vis Sci. 2005;82(4):273-278.
- Jones LA, Sinnott LT, Mutti DO, et al. Parental History of Myopia, Sports and Outdoor Activities, and Future Myopia. Invest Ophthalmol Vis Sci. 2007;48(4):1678-1685.
- Zadnik K, Sinnott LT, Cotter SA, et al.; CLEERE Study Group. Prediction of Juvenile-Onset Myopia. JAMA Ophthalmol. 2015;133(6):683-689.
- Ekdawi NS, Nusz KJ, Diehl NN, Mohney BG. The development of myopia among children with intermittent exotropia. Am J Ophthalmol. 2010;149(3):503-507.
- Rose KA, Morgan IG, Ip J, et al. Outdoor activity reduces the prevalence of myopia in children. Ophthalmology. 2008;115(8):1279-1285.
- He M, Xiang F, Zeng Y, et al. Effect of time spent outdoors at school on the development of myopia among children in China: a randomized clinical trial. JAMA. 2015;314(11):1142-1148.
- Xiong S, Sankaridurg P, Naduvilath T, et al. Time spent in outdoor activities in relation to myopia prevention and control: a meta-analysis and systematic review. Acta Ophthalmol. 2017;95(6):551-566.
- Huang HM, Chang DST, Wu PC. The association between near work activities and myopia in children — a systematic review and meta-analysis. PLoS One. 2015;10(10):e0140419.
- Donovan L, Sankaridurg P, Ho A, et al. Myopia progression rates in urban children wearing single-vision spectacles. Optom Vis Sci. 2012;89(1):27-32.
- Kurtz D, Hyman L, Gwiazda JE, et al. Role of parental myopia in the progression of myopia and its interaction with treatment in COMET children. Invest Ophthalmol Vis Sci. 2007;48(2):562-570.
- Loh KL, Lu Q, Tan D, Chia A. Risk factors for progressive myopia in the atropine therapy for myopia study. Am J Ophthalmol. 2015;159(5):945-949.
- Mutti DO, Sinnott LT, Brennan NA, et al.; CLEERE Study Group. The Limited Value of Prior Change in Predicting Future Progression of Juvenile-onset Myopia. Optom Vis Sci. 2022;99(5):424-433.
- Hyman L, Gwiazda J, Hussein M, et al. Relationship of age, sex, and ethnicity with myopia progression and axial elongation in the correction of myopia evaluation trial. Arch Ophthalmol. 2005;123(7):977-987.
- Luong TQ, Shu YH, Modjtahedi BS, et al. Racial and Ethnic Differences in Myopia Progression in a Large, Diverse Cohort of Pediatric Patients. Invest Ophthalmol Vis Sci. 2020;61(13):20.
- Bullimore MA, Brennan NA. Myopia Control: Why Each Diopter Matters. Optom Vis Sci. 2019;96(6):463-465.
- Ip JM, Saw SM, Rose KA, et al. Role of near work in myopia: findings in a sample of Australian school children. Invest Ophthalmol Vis Sci. 2008;49(7):2903-2910.
- Wildsoet CF, Chia A, Cho P, et al. IMI – Interventions for Controlling Myopia Onset and Progression Report. Invest Ophthalmol Vis Sci. 2019;60(3):M106-M131.